FUE vs DHI: What’s the Difference Between These Hair Transplant Techniques?
If you’re considering a hair transplant, chances are you’ve come across two popular techniques: FUE (Follicular Unit Extraction) and DHI (Direct Hair Implantation). While both offer effective and natural-looking results, each method has its own unique approach and advantages.
In this article, we’ll break down the key differences between FUE and DHI, helping you make an informed decision about which hair restoration method is right for you.
🔍 What Is FUE (Follicular Unit Extraction)?
FUE is one of the most widely used hair transplant techniques today. In this method:
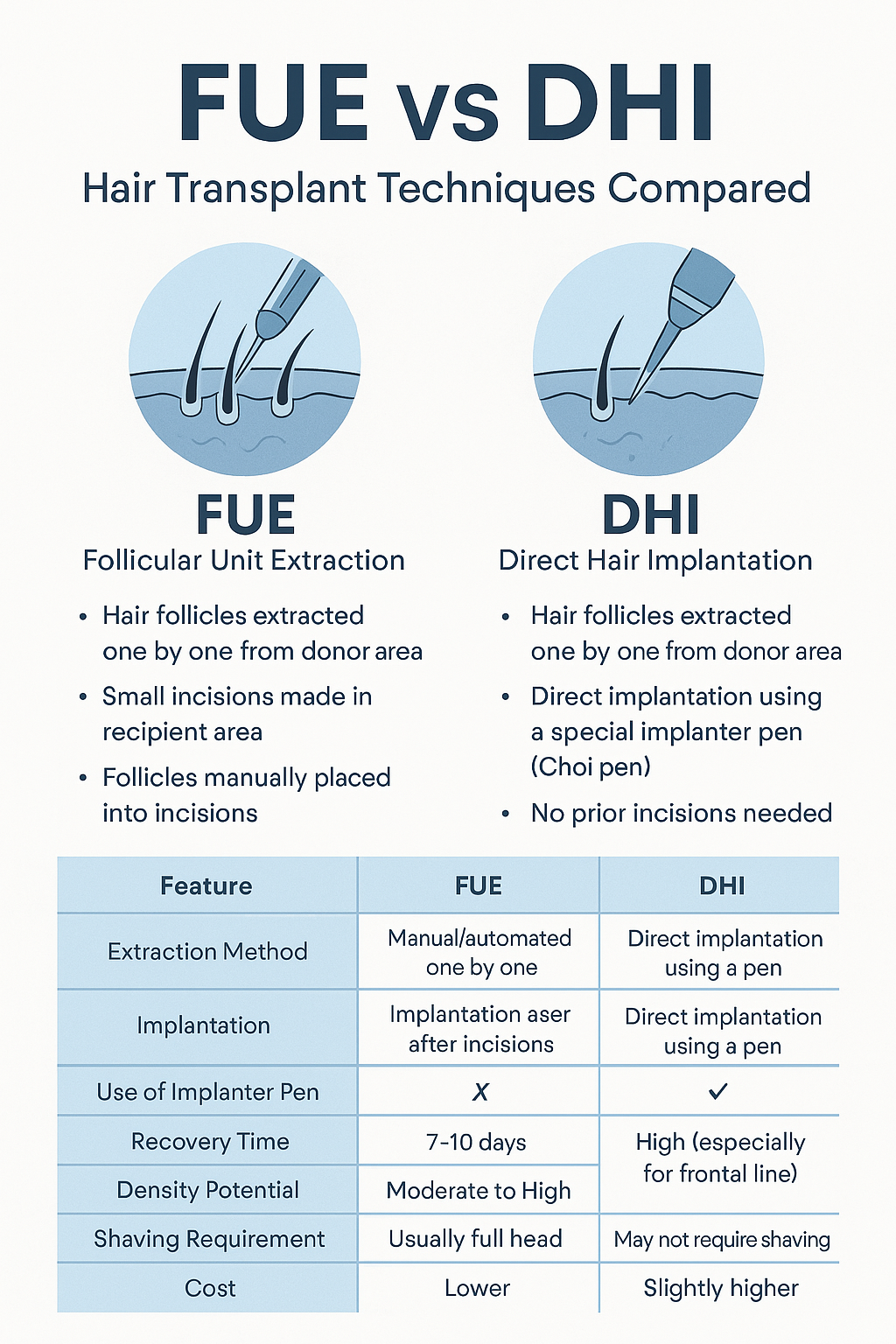
Hair follicles are extracted one by one from the donor area (typically the back of the scalp).
Small incisions are made in the recipient area before implantation.
The extracted follicles are then manually placed into the incisions.
![]()
Benefits of FUE:
Minimally invasive with no visible scarring
Fast recovery time
Suitable for larger transplant areas
No stitches required
💡 What Is DHI (Direct Hair Implantation)?
DHI is a more recent and advanced technique. It builds on FUE but with a key difference in implantation:
Hair follicles are extracted similarly to FUE.
Instead of creating incisions first, a special implanter pen (Choi pen) is used to simultaneously open the channel and implant the follicle.

Benefits of DHI:
Higher precision and control over angle, depth, and direction
Denser and more natural-looking results, especially in the hairline
Less bleeding and faster healing in some cases
No need to shave the recipient area (in certain cases)
🆚 FUE vs DHI: Key Differences at a Glance
| Feature | FUE | DHI |
|---|---|---|
| Extraction Method | Manual/automated one by one | Manual/automated one by one |
| Implantation | Manual placement after incisions | Direct implantation using a pen |
| Use of Implanter Pen | ❌ No | ✅ Yes |
| Recovery Time | 7–10 days | 5–7 days |
| Density Potential | Moderate to High | High (especially for frontal line) |
| Shaving Requirement | Usually full head | May not require shaving |
| Cost | Lower | Slightly higher |
🧠 Which One Is Right for You?
Both techniques are effective, but your choice depends on:
Your hair type and goals
The size and area of baldness
Whether you want higher density in specific areas (e.g., hairline)
Your budget and recovery expectations
👉 FUE may be better for larger areas and patients seeking a quicker, more affordable solution.
👉 DHI might be ideal for those focusing on hairline restoration and maximum density.
📌 Final Thoughts
Both FUE and DHI hair transplant techniques offer excellent, permanent results when performed by skilled professionals. The best method for you depends on your unique hair characteristics, expectations, and medical advice.
Before deciding, schedule a consultation with an experienced hair transplant clinic to evaluate your options.